Why not? Companies that make pharmaceuticals, prosthetics, imaging devices, etc are all on the stock market too, so if hospitals weren’t on there, you could build a portfolio to approximate it by buying producers of medical equipment.
The real issue isn’t whether something is publicly traded, but collusion between groups to keep prices high. For example, it’s mutually beneficial for insurance, hospitals, and medical equipment providers to increase costs. Higher equipment costs means care providers can charge more (what’s another few hundred when the bill is in the thousands?), and higher total bills means insurance companies can charge higher premiums (they’re usually limited to a certain percent of cost as profit). Hospitals generally don’t have direct competitors since it’s prohibitively expensive to build one and there’s lots of bureaucracy based on “need,” so you can’t just go next door to an org that’s not involved in the collusion.
There are lots of viable solutions here, but banning them from the stock market isn’t going to solve anything. The first order of business imo is making everything more transparent.
I know it’s an anecdote, but I have a coworker that shared an experience moving from Canada to the US, and they said they much prefer the American healthcare system to the Canadian system. This is from the perspective of a relatively well off individual (not rich, just middle to upper middle class), so obviously someone at the bottom end of the income spectrum would have a different opinion.
So my question for people who promote socialized medicine is this: if you could easily afford both, would you prefer socialized or privatized medicine? And why?
I think we have a cost problem, not a structural problem, so we should look at ways of reducing cost before completely changing the structure of our healthcare system. My primary concern is getting insurance away from employers, publicly funding emergency services, and making hospital costs more transparent (e.g. publicly posted price ranges for common procedures). As in, reform the current system, not replace it.
know it’s an anecdote, but I have a coworker that shared an experience moving from Canada to the US, and they said they much prefer the American healthcare system to the Canadian system. This is from the perspective of a relatively well off individual (not rich, just middle to upper middle class), so obviously someone at the bottom end of the income spectrum would have a different opinion.
The problem is that healthcare systems are meant to take care of the entire population, not just the middle class or higher. If you are a moderately healthy and wealthy person, yes the American healthcare system is fine, but that’s not exactly the what your entire system should be geared for.
The only reason they like the system is because they are the bread and butter of private insurance. Healthy working adults whom don’t require lots of expensive care. However, if they were to developed a chronic illness, or get injured or I’ll to the point where they can’t maintain their employment… That’s when you get to experience the worst healthcare experience America has to offer.
if you could easily afford both, would you prefer socialized or privatized medicine? And why?
As someone who’s had socialized medicine (Tricare) and now currently has “good” private insurance (BCBS ppo), I definitely prefer socialized.
There’s no worry that your going to catch an unexpected co-pays, you aren’t nickle and dimed for every script or visit. No worrying about out of pocket maximums, yearly deductibles, or lack of specific coverage. You don’t have to get specialized insurance for just your eyes and teeth, the benefits go on and on.
I think we have a cost problem, not a structural problem, so we should look at ways of reducing cost before completely changing the structure of our healthcare system.
The cost problem stems from the structural problem. Private insurance steals the ability to effectively collectively bargain for lower prices. It also diverts funding away from the socialized insurance pool of Medicare, which lacks the young healthy subscribers that help stabilize and fund the care for elderly and sick.
Imagine if all the money that private insurance pockets went towards actually caring for people. Imagine if hospitals didn’t have to employ a small army of managers and billing agents, just to get paid for services already rendered. Imagine the collective bargaining power that we’d all have if pharmaceutical companies knew there was only one customer in the entire nation.
You give that all away for what? A policy that goes away the moment your employer decides they don’t want to pay that much this year? A policy that ties your physical well being to your employment? A policy that terminates your coverage the very moment you need it the most?
unexpected co-pays, you aren’t nickle and dimed for every script or visit
Again, you’re talking about cost, not which you’d prefer from a service perspective.
I think there are lots of opportunities to make costs lower, such as reducing patent lengths (reduces medication costs) and simplify insurance (reduces admin costs). We should also make changes to liability law so doctors can focus on providing care. Some specific proposals:
patents - reduce to 5-7 years; should cut costs of pharmaceuticals
insurance - simplify and standardize coverage; coverage details and bill processing should be automated
publicly post costs of common procedures, and give expected, average, and maximum costs before any procedure
And so on. And on top of that, expand Medicare/Medicaid a bit with costs phasing in the higher your income goes. I think we should also cap access to Medicare for retirees at a certain income level as well, and remove FICA tax caps.
We should absolutely be discouraging employer sponsored insurance and encouraging longer term insurance plans (e.g. like life insurance, you lock in at a lower rate if you sign up while healthy). Dropping someone from insurance shouldn’t be a thing at all, and the payout for doing so should be much higher than any costs the insurance company would incur by keeping them.
Again, you’re talking about cost, not which you’d prefer from a service perspective.
If you went to a restaurant and they ran separate charges every time you ordered something… You wouldn’t consider that bad service?
Also, I went to the same physician when on Tricare, so it’s the same exact service, minus all the billing hassle.
I think there are lots of opportunities to make costs lower, such as reducing patent lengths (reduces medication costs) and simplify insurance (reduces admin costs).
And I think you could do the same things and still lower the cost even more by banning privatized insurance?
Also, what is the profit motive for insurance companies to simplify their process? Their systems were purpose built to be as complicated and time consuming as possible, if they make the process easier, their subscribers would utilize it more, making insurance pay more often.
patents - reduce to 5-7 years; should cut costs of pharmaceuticals
insurance - simplify and standardize coverage; coverage details and bill processing should be automated
And again, why would corporations do this? And how would we enforce this?
The Medicare billing is automated, and pretty simple. It’s what every insurance company has the option of doing, but only Medicare and Medicaid have automated the process. This is because private insurance companies have no profit motive to pay for their prescribers healthcare.
publicly post costs of common procedures, and give expected, average, and maximum costs before any procedure
Most hospitals have this information available, especially if you call their financial services office. In fact if you are a Medicare patient this information is publicly available on the CMS website, and they list exactly how they came to that figure.
The whole hidden ledger thing is primarily only a problem at privatized hospitals that were bought or built by private hospital networks operating for profit.
I think we should also cap access to Medicare for retirees at a certain income level as well, and remove FICA tax caps.
The inherent problem with this is that the elderly are fundamentally uninsurable. You can’t make a profit from an elderly subscriber, the cost of their end of life care will always cost more than any subscription fee they may pay in.
This is why the vast majority of private insurance do not offer primary insurance to people older than 65. The whole point of private insurance is to extract money from healthy patients and then dump them onto Medicaid if they become disabled, or onto Medicare when they begin to age and decline in health.
We should absolutely be discouraging employer sponsored insurance and encouraging longer term insurance plans (e.g. like life insurance, you lock in at a lower rate if you sign up while healthy).
Who would offer those plans, and why? The only reason most people can afford private insurance is because their employer collectively bartered for the price. A lot of people have no idea how much of their employee compensation package is taken up by their insurance, but the burden of cost is redistributed by the entire employer pool.
Dropping someone from insurance shouldn’t be a thing at all, and the payout for doing so should be much higher than any costs the insurance company would incur by keeping them.
This would bankrupt private insurance companies…
I don’t think you fully understand how hard it is to make money on health insurance. The only way to do so is by withholding healthcare to your subscribers, or to offer plans with obscene co-pays or deductible.
The cost on average for full coverage is around 8.5k dollars a year for an individual, or 24k for a family. Meaning that the cost of a single operation, illness, or inpatient procedure will wipe away the potential profits from an individual subscriber for years. The only way to recover from having one I’ll subscriber is to balance them with a dozen healthy subscribers.
Without managing this equation of large healthy profitable pool vs small costly pool, the entire charade of private insurance would collapse upon itself.
One of the largest drivers in the increase in healthcare cost is these types of people. People whom don’t have any insurance, but still have healthcare needs. For these people the emergency room is typically their only option. This is one of the reasons emergency medicine is such a drain on hospital resources. For every person they treat without insurance, they have to raise the cost on people with insurance, simply so they don’t go out of business.
It’s funny you mention restaurants, in that case I don’t particularly care when they bill me because the menu says precisely what I’ll pay (counter order vs table service doesn’t matter as much as cost and quality). If it’s market rate (steak or seafood), they’ll tell me what the day’s rate is and what cuts they have.
I don’t get that with health care, even getting a range in a quote is like pulling teeth. I pushed back a ton when my daughter needed a surgery, and after several calls I still didn’t get a clear answer, and this was for a routine surgery. The quality and speed of service was great, billing was not.
One of the benefits of socialized medicine is not having to worry about billing, but you also often get delays in care. I don’t think we need to go to socialized medicine to solve the unexpected costs issue, we can expect care providers to absorb some of the variability.
what is the profit motive for insurance companies to simplify their process?
I agree, the current profit motives are misaligned, and pushes like the ACA to further expand the number of people with insurance further entrench these practices.
The profit motive should be attracting customers who otherwise would go without. But since pricing isn’t transparent, cash payers don’t have the same leverage to get a fair price. Many care providers have an informal “cash discount,” but that’s just not the same.
If the system works well for cash customers, insurance would need to earn customers’ business, but when most people have insurance, the patient is no longer the customer, the employer is, so they’ll charge individual customers more than employers with group plans. If we separate the insurance from the employer, they would need to cater to patients.
Removing private insurance is one option, but that’s also quite disruptive and has potential for other issues (e.g. why would Medicare bother with good customer service if it’s the only option?).
Most hospitals have this information available
That wasn’t my experience. We had two options for a surgery with different risks and costs, and after several calls, we couldn’t get any numbers, just A costs more than B. That’s why I’m so interested and “it depends on your insurance” blah blah blah. That’s why I’m so interested in this. And this wasn’t some podunk hospital, it was the premier children’s hospital in the state, run by the premier public university in the state, and services kids outside the state.
I should be able to get quotes on a procedure from multiple care givers for a non-urgent procedure (like the one we had).
how would we enforce this?
Patients should be able to switch insurance if they don’t like the one they have. Right now, you either use the insurance you have or pay out the nose by giving up company cost share and ACA subsidies.
If my company offers a crappy plan, I should be able to take what they would’ve contributed and pick my own plan. If that was the case, insurance companies would try harder to make their service more convenient, just like auto insurance does (not a gold standard, but much better), and HR orgs would probably try harder to pick better plans.
You can’t make a profit from an elderly subscriber, the cost of their end of life care will always cost more than any subscription fee they may pay in.
If you’re wealthy, you don’t need much from your insurance. End of life care could be self funded, and insurance is there for the other surprises that could ruin your retirement. It would be totally acceptable for an insurance company to require some kind of down payment to cover EOL care, or a minimum number of years for coverage (if you die before the end of the contract, it counts as debt the estate needs to pay back).
their employer collectively bartered for the price
I’ve run the numbers and can get a similar price (within 10% or so) for similar coverage without ACA subsidies, but I need to factor in how much they’d contribute to their own plan. Add to that couples who both work, your options are: have separate plans (less efficient) or give up the employer subsidy.
This would bankrupt private insurance companies
No, they’d just adjust rates to compensate. If there’s something insurance companies are good at, it’s averaging costs and holding a surplus. So a company that’s better able to estimate this should get more customers and stay in business longer.
If they offer a 10-year or longer plan, they just need to average costs across their target demographic over those years to come up with a premium. Term life insurance companies do this, so why not health insurance?
For these people the emergency room is typically their only option.
Especially for homeless people. Which is a huge part of why I’m a fan of government funded ER. That’s a huge risk factor for insurance companies and hospitals, and it’s also a huge complexity for visitors and whatnot, so it should just be provided. If the paramedic thinks you need emergency care, it should be 100% free. However, hospitals should be empowered to deny care (and charge for wasting ER capacity) for non-emergencies.
But any extended care once you’re stabilized should be covered by insurance instead, because you have actual choices in your care (and could theoretically walk out if you choose not to accept further care).
It’s funny you mention restaurants, in that case I don’t particularly care when they bill me because the menu says precisely what I’ll pay (counter order vs table service doesn’t matter as much as cost and quality). If it’s market rate (steak or seafood), they’ll tell me what the day’s rate is and what cuts they have.
We were talking about service, not cost… Like if they ran your card for every individual item, as soon as you ordered it. “I’d like to start with a coke to drink” takes out card to charge. “Then I’d like a starter” takes out card.
This is what i mean by bad service.
don’t get that with health care, even getting a range in a quote is like pulling teeth. I pushed back a ton when my daughter needed a surgery, and after several calls I still didn’t get a clear answer, and this was for a routine surgery. The quality and speed of service was great, billing was not.
This is likely because you called before a prior authorization was completed, meaning that you most likely were utilizing private insurance. If you were utilizing Medicaid, which doesn’t require pre authorization, then it would be really simple to tell you.
You can’t give an accurate quote for private insurance because the individual plans are so personalized by their workplace or insurance brokers to lower cost and coverage that we literally don’t know what your coverage until we submit if for authorization and equate for things like deductables and copay.
This authorization process requires not only a referral, but an itemized script, supporting notes, and a face to face with the provider. So unless they had the opportunity to complete these task, private insurance doesn’t allow us to give you a quote.
but you also often get delays in care.
Lol, you were just talking about a delay in care due to billing issues with private insurance. American private insurance also has the same exact delays in care, waiting weeks for prior auth, waiting months for people to meet their deductible, avoiding needed care because of cost, and just plain waiting for specialized care because we don’t have enough specialty providers. Many specialty providers like neurologist or or rheumatologist have left the field specifically because of paperwork burnout. The authorization process for these expensive specialty practices is so scrutinized by insurance companies that it can take months of daily negotiation to even see a patient.
I agree, the current profit motives are misaligned, and pushes like the ACA to further expand the number of people with insurance further entrench these practices.
Lol, wrong again. The plans allowed on the aca marketplace had to follow aca guidelines, which included automating the billing process. These platinum, silver, and bronze plans are actually pretty easy to work with compared to those offered by people’s workplaces. In the beginning we were actually pretty excited to see actual changes to the system, however since the removed mandate, and the subsequent deterioration of coverage in these plans, it’s rare to see patient actually utilize there benefits.
The profit motive should be attracting customers who otherwise would go without. But since pricing isn’t transparent, cash payers don’t have the same leverage to get a fair price. Many care providers have an informal “cash discount,” but that’s just not the same
What are you talking about about? Why would an insurance company want to attract uninsured people? The uninsured people of America are some of the most at risk communities in America. They are impoverished, underemployed, and are disproportionately likely to have long term health conditions. There is no wealth to extract from these people, and the longer they have been uninsured, the more likely they are to require excessive care once they are insured.
If the system works well for cash customers, insurance would need to earn customers’ business, but when most people have insurance, the patient is no longer the customer, the employer is, so they’ll charge individual customers more than employers with group plans.
Lol, you have no idea the average cost of healthcare people accumulate during their lifetimes. One serious stint at an inpatient facility would bankrupt a wealthy person. As I said, there is no profit in healthcare that isn’t created by denying healthcare.
Removing private insurance is one option, but that’s also quite disruptive and has potential for other issues (e.g. why would Medicare bother with good customer service if it’s the only option?).
Why exactly would it be quite disruptive? Also, Medicare is the only option for the people who have it… If you qualify for Medicare for your primary insurance, private insurance automatically becomes your secondary. Medicare still offers more coverage than any other private plan. I don’t think you quite understand that the people whom work in healthcare do so because they want to help people. Being a physician doesn’t exactly mean you’re making the big bucks anymore. There are plenty of fields that require a lot less schooling and pay way more.
That wasn’t my experience. We had two options for a surgery with different risks and costs, and after several calls, we couldn’t get any numbers, just A costs more than B.
As I said previously, this is an inherent problem created by private insurance. You can’t just call and shop around on private insurance, the way they set up the prior authorization process is expressly made to prohibit this. The only way to do this is to call your insurance as a subscriber, and talk to your plans agent. They will direct you to their preferred network, where they have negotiated cost previously.
Again, insurance companies purposely create inefficient and archaic systems so their customers won’t utilize their services as often. They make us do all the explaining and processing, so we get the blame.
should be able to get quotes on a procedure from multiple care givers for a non-urgent procedure (like the one we had).
I agree, and if your child was on Medicaid it would have been super easy… You would have been told $0.00. Medicaid is an actual healthcare system, and because their goal is to actually improve their patients health it functions as intended.
Patients should be able to switch insurance if they don’t like the one they have.
Right, but who is preventing people from switching plans…
Oh yeah, private insurance. Because private insurance cannot afford to have patients switching insurance every time a patient has an operation. How are you going to remain solvent if a subscriber can just run up cost and then switch to a different insurance pool without contributing?
my company offers a crappy plan, I should be able to take what they would’ve contributed and pick my own plan. If that was the case, insurance companies would try harder to make their service more convenient, just like auto insurance does (not a gold standard, but much better), and HR orgs would probably try harder to pick better plans.
You are ignoring the fact that private insurance is a gamble. It’s a company gambling that you as an individual will contribute more to the insurance pool than you take out before you turn 65. If a person can just switch insurance companies they could just change plans every year they needed an expensive operation. The same can be done with home/car insurance, but car/home insurance is allowed to charge people with prior history of heavy utilization with higher fees and deductible. This is not legal in healthcare, as it would automatically price out people with chronic illnesses.
If you’re wealthy, you don’t need much from your insurance.
And how many people are wealthy compared to the amount of people who are poor? Is your solution to build the entire country’s healthcare system for 5% of the population? Also, why should your life savings be eaten up by healthcare cost if you already paid for life insurance your whole life? I just don’t see why you are so ardent about paying more money for less coverage?
I’ve run the numbers and can get a similar price (within 10% or so) for similar coverage without ACA subsidies,
You are comparing individual self funded plans to those offered by your work? As someone who owns a company and works for a hospital… I highly doubt that. I’m still utilizing my hospital insurance because the self funded ones offered to small companies were quite a bit higher when factoring in deductible and copays. If you were talking about individually funded plans, I would urge you too re examine the coverage.
they’d just adjust rates to compensate.
The amount they would have to raise rates exceeds their clients ability to pay… You can’t squeeze blood from a stone, and people are already struggling with their current cost. Raising the rate high enough to account for chronic disabilities isn’t an option. This is why they fought so hard against the law that prevented them from rejecting coverage for people with conditions like type 1 diabetes, which isn’t a disability that qualifies for Medicaid, but has a high cost.
Which is a huge part of why I’m a fan of government funded ER. That’s a huge risk factor for insurance companies and hospitals, and it’s also a huge complexity for visitors and whatnot, so it should just be provided.
That’s just a bandaid who’s only function is to protect insurance companies. If insurance companies are not good enough to cover emergent healthcare what’s their point? If you can get free healthcare at emergency rooms instead of being insured, why not just go to the ER? This would just make the emergency room problem worse.
Why spend so much time coming up with worse work arounds when you haven’t been able to tell me a single advantage private insurance brings to the table?
service, not cost… Like if they ran your card for every individual item
I’m not really following the point of the analogy.
If cost doesn’t matter, I’d just give them my card and they can run it as often as they like. That’s basically how it works on cruise lines, you set up a payment system and they scan your cruise card with each transaction. It’s not an issue at all.
individual plans are so personalized
Right, and that’s because the policy holder usually isn’t the customer, the employer is.
Health insurance would likely be a lot simpler if the average policy holder could switch insurance, especially if there’s no open enrollment period (like car insurance, I can shop rates anytime and understand what I’m buying pretty easily).
delay in care due to billing issues with private insurance
No, there was no delay in care. Once I picked the option, I got the procedure done in the next week or two.
The only delay was because I wanted the quote before picking the solution, and that’s a totally artificial limitation that can be fixed by changing how insurance works (i.e. give me the cash price, and I’ll figure in the deductible and whatnot).
You’re right, the problem is paperwork, which is why we should give the insurance companies fewer options to reject claims. Eliminate or automate the authorization step. Care providers should never need to talk to anyone at the insurance company.
Why would an insurance company want to attract uninsured people?
Higher risk just means higher costs. They can still collect some percentage of premiums, so why would they turn it down?
you have no idea the average cost of healthcare people accumulate during their lifetimes
You’re right, and those numbers are hard to come by since most studies/articles assume Medicare in retirement and focus on out of pocket costs. If I was proposing actual policy, I’d do my due diligence, but for this kind of discussion, I use what’s readily available.
65+ insurance is indeed unique, hence why I mentioned an escrow system. Basically, you prepurchase insurance including end of life care. That amount of money buys you a certain guaranteed tier of end of life care, even if your individual costs exceed that. I’m guessing that escrow is something like $300-500k for basic EOL care, plus some extra for routine medical care. But I only have mediocre data to work from. If you have a good source, I’m interested.
I don’t know how practical it is, it’s just an idea for an alternative to Medicare for the wealthy. But honestly, just uncapping income for paying in and expanding Medicare a bit for poorer people is probably more reasonable.
I don’t think you quite understand that the people whom work in healthcare do so because they want to help people
Sure, and the same is true for education. And the problems with both are pretty similar:
they’re restricted in how they do their jobs
there’s a lot of paperwork, and paperwork sucks
there absolutely is a point where the career isn’t worth it
In many areas, the government has a near monopoly on education, yet the problems persist. Why should we expect medicine to be much different? Once government has a near monopoly on something, it becomes very political.
Maybe something like the public option doesn’t have as many tradeoffs, IDK, but socialized medicine certainly would. I’d only be in favor of a public option if care providers received the same amount from cash customers vs Medicare customers, and that amount is transparent and publicly auditable (i.e. if Medicare wants to fight high prices, that should benefit cash customers). That doesn’t happen today with the privatized system, so that’s where my focus is.
Privatized insurance isn’t the goal here, privatized medicine is. If we want to subsidize that for the poorer end of the income range, I’m fine with that, but the majority should be expected to pay for a large portion of medical care, otherwise market forces don’t work properly.
insurance companies purposely create inefficient and archaic systems so their customers won’t utilize their services as often
They do it because it doesn’t cost them customers. I can’t vote with my wallet and switch my insurance, I can only beg my HR department to offer something different. I am not the customer here.
Many customers are willing to pay a bit more in other industries to avoid BS, I don’t see why that should be any different for health insurance.
The reason we have the system we do is because government incentivizes company-provided health insurance. We should instead encourage people to select their own plans. The ACA increases barriers to rejecting company insurance and doubles down on involving employers in health insurance decisions.
Either we need to completely put patients in control of their insurance or provide it as a public good. The current middle ground is worse than either extreme imo.
they could just change plans every year they needed an expensive operation
Auto insurance seems to work just fine with this. If I make lots of claims with one insurer, that slate won’t just be wiped clean with the next one.
If customers can easily switch, that should encourage insurance companies to lock in customers with longer term policies to spread out the risk.
And insurance isn’t really a gamble, it’s actually quite the opposite, a way to reduce risk. The insurance company doesn’t expect any particular individual customer to be profitable, they just expect that their customers will be profitable on average. Individuals buy insurance knowing that they statistically don’t get value from the insurance, they’re merely getting it to reduce their own financial risk. For an insurance company, it’s like buying an index fund instead of individual stocks, and for individuals it’s like buying an annuity instead of stocks.
You are comparing individual self funded plans to those offered by your work?
Yes. I’m comparing individual, non-subsidized ACA plans with those offered by my work. My work only offers high deductible plans with a premium and HSA contribution, and I’m comparing against ACA HSA plans with a similar deductible and max out of pocket. I’ve never had a copay, everything has been a relatively simple deductible.
Specific details certainly differ, but I think it gets me in the ballpark.
And this is for a reasonably large company. We have something like 3000 employees, so it should be big enough to benefit from collective bargaining. I haven’t run the numbers for a couple years (I compared ACA when self-employed vs new company), so things could have changed. I like this method because costs are both transparent, and I actually estimate my costs (and subsidy) if i decide to stop working in a spreadsheet. I’m certainly no expert, but I do try to be reasonably thorough.
And yeah, I’ll probably redo the numbers soon. I generally do this around tax season because I like to estimate my taxes to see how close I am (was really close last year), and I have a section to compare expected total costs of care for the two plans my company offers (only difference is deductible, premium, and max out of pocket) and a comparable ACA plan (those numbers are publicly available). Specific plan details vary, and it’s not something I can get super accurate with (how do you put a price on a procedure I’m unlikely to need?), but hopefully it’s close.
If you’re interested, maybe I’ll run the numbers this weekend and reply with the details. I’m not a medical or insurance expert, but I am very interested in personal finance and actually enjoy spending a few hours crunching numbers.
The amount they would have to raise rates exceeds their clients ability to pay
Maybe. But that’s also assuming healthcare costs stay stagnant. If we drastically reduce the complexity of dealing with insurance, we also reduce the costs to insurance, which may be enough to offset an increase in claims.
All the paperwork is waste, and it’s getting to be a massive problem, but it suffers from a prisoner’s dilemma-type issue (an individual company is better off complicating the process in the short term, but if everyone does that, net costs go up) so the current setup won’t resolve itself.
If insurance companies are not good enough to cover emergent healthcare what’s their point?
Insurance companies exist to cover extreme financial burdens, like developing cancer or other chronic conditions. Basically, things that could bankrupt you.
The issue with ER is that it often goes against your will, and getting financial consent could be the difference between life and death. What are you going to do if insurance rejects your claim? What if someone else calls an ambulance for you and you can’t pay? What if you’re a tourist and you don’t understand the US medical system? There’s just way too many weird cases to the point where we can’t just expect insurance companies to take the hit here.
Publicly funded ER solves those problems and can protect emergency care providers from lawsuits and whatnot so they can focus on providing care. Once the patient is stabilized, they can make decisions for ongoing care, and that’s where insurance should get involved.
In general, if something is involuntary or a natural monopoly, it should be publicly provided. That’s absolutely the case for emergency care (I can’t pick the ambulance company someone else calls for me). But routine and chronic care absolutely is voluntary and isn’t a natural monopoly.
If you can get free healthcare at emergency rooms instead of being insured, why not just go to the ER?
The ER would reject you and potentially fine you for nonemergency care. Just like calling 911 for non-emergencies.
The real issue isn’t whether something is publicly traded, but collusion between groups to keep prices high. For example, it’s mutually beneficial for insurance, hospitals, and medical equipment providers to increase costs. Higher equipment costs means care providers can charge more (what’s another few hundred when the bill is in the thousands?
This isn’t how pricing is set for medical equipment… Nor is high equipment cost the reason behind the pricing increase.
Every hospital that accepts Medicare utilizes CMS guidelines when it comes to billing. Medicare sets the general price for items, factoring in things like historic pricing, cost of purchase from vendor, and the price of labour required to fit or make the device function.
The complex and expensive aspect of hospital billing stems from the introduction of private insurance companies. The ones that require more paperwork and processing time than Medicare, and will attempt to make the process as hard as possible.
Hospitals generally don’t have direct competitors since it’s prohibitively expensive to build one and there’s lots of bureaucracy based on “need,” so you can’t just go next door to an org that’s not involved in the collusion.
Because hospitals are a natural monopoly, not only are they prohibitedly expensive, but it’s also extremely hard to profit from them in the long term. Which is why there’s a large amount of bureaucracy to get them built.
Pretty much every ER room in America is a huge money sink that the rest of the hospital has to economically support. You add too many hospitals, and the services that are profitable get too spread across the area to support their individual ER operations.
Which is why about 10-15 years ago there was a large push from venture capital to build “hospitals” without trauma rooms. These hospitals began to eat up all the funding in the area and began shutting down hospitals with trauma wards. This is when a lot of states adopted legislation that would help curb this behavior.
There are lots of viable solutions here, but banning them from the stock market isn’t going to solve anything. The first order of business imo is making everything more transparent.
Banning private insurance is the only thing that would lower prices for Americans. None of the issues you covered are even close to the reason why things are getting expensive.
private insurance companies. The ones that require more paperwork and processing time
But what are those insurance companies processing? If you look at it, it’s “special deals” so the agents can get a bonus, it has nothing to do with actually saving their customers money. Hospitals inflate prices so they have room to make cuts so the insurance sales people feel like they’re winning.
The problem here isn’t with the nature of insurance, but the collusion between insurance companies and care providers. It’s a dance they play so everyone feels like they’re winning, and at the end of the day the customer is the one that loses. It’s not a competitive market, it’s a bureaucratic one where you have HR departments, insurance salespeople, and hospitals all propagating the current system because it’s lucrative for all of the middlemen.
Medical suppliers want a piece of the action too. That’s why we get things like insulin prices going up:
The high cost can be attributed in part to “evergreening,” a process in which drug companies make incremental improvements to their products that can extend the life of their patents, said Dr. Kevin Riggs, a physician at the University of Alabama at Birmingham Heersink School of Medicine. He co-wrote a study published in the New England Journal of Medicine in 2015 that described the century-long history of the drug.
They prevent competition through the patent and regulatory systems, and hospitals and insurance companies are fine with it because they just pass the costs on to the consumer. Consumers don’t really have a choice because most insurance comes from employers (who just pay employees less to compensate) or taxes (ACA subsidies). Nobody actually pays the full price, so the system continues.
The same goes on with medical devices, but volume is much lower so it’s easier to prevent real competition. Add to that the legal risk for choosing a cheaper product if anything goes wrong and you’ll find no incentive to cut costs.
Let’s assume we eliminate private insurance, you just change the private collusion to public collusion, and instead of middle managers getting paid in the public sector, you get political favors to keep prices high (e.g. campaign donations). Moving insurance from private to public just moves money from one pocket to another. The true solution here is to expose the collusion, not politicize it. If you want proof of this in action, look no further than the defense department in the US.
Pretty much every ER room in America is a huge money sink that the rest of the hospital has to economically support
Which is because of free riders. The solution to that problem is different: emergency care should be completely publicly funded. It’s so expensive because the hospital has to deal with people skipping on their bills and just move the costs to paying customers.
I think we should make ambulances and all non-elective care completely free, provided a paramedic recommends emergency care.
Natural monopolies aren’t intrinsically changed by demand…
But what are those insurance companies processing?
It’s not the insurance company that is doing the processing. It’s the hospitals, they have to hire more and more billing agents just to extract the money that the insurance has already agreed to pay.
special deals" so the agents can get a bonus
Lol, no. By “special deals” you mean 20% less than the Medicare allowable, and if you don’t agree then you are no longer in network.
Hospitals inflate prices so they have room to make cuts so the insurance sales people feel like they’re winning.
No, they inflate the prices so that when insurance companies ask for less money it doesn’t bankrupt the hospital.
The problem here isn’t with the nature of insurance, but the collusion between insurance companies and care providers.
You have no idea what you are talking about about… I’m a provider at a hospital, specializing in orthopedics and rehabilitation. I’ve never spoken to an insurance agent about pricing. That’s not how it works.
Medical suppliers want a piece of the action too. That’s why we get things like insulin prices going up:
Those are pharmaceutical companies, not medical suppliers, they are billed under completely different systems…
Also, the reason insulin pricing is so high is because Medicare isn’t allowed to barter for pricing, largely in part because it would be unfair to private insurance companies who have smaller subscriber groups.
we eliminate private insurance, you just change the private collusion to public collusion, and instead of middle managers getting paid in the public sector, you get political favors to keep prices high (e.g. campaign donations). Moving insurance from private to public just moves money from one pocket to another.
Oh yeah, I forgot how every medical system on the planet was completely fraudulent… Oh wait, nope, mainly just America.
The biggest way to improve pricing is by group bartering, which is how every other 1rst world nation pays less for medical equipment, treatment and prescription cost than the US.
Again, nothing you said was accurate, and anyone who takes it as so is now dumber than when they began reading. Please stop spreading misinformation about fields of study you do not specialize in.
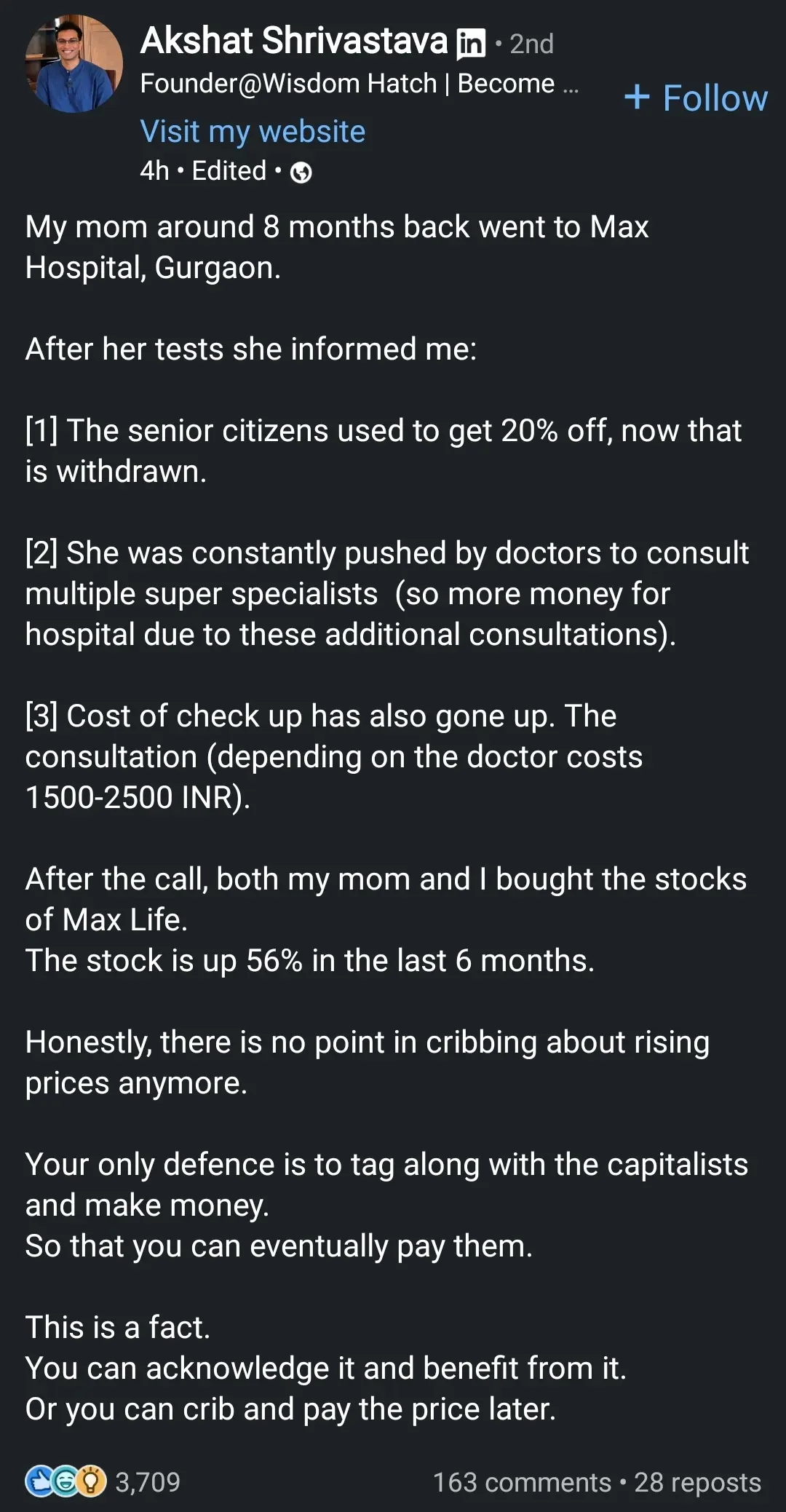
Market competition is fine, but corporations are specifically obligated to focus on profits over other considerations, and in this case that is inappropriate and creates perverse incentives. Consider people like in the OP who have cynically bought in (or are in some retirement fund that bought in on their behalf) and now their financial wellbeing depends on hospitals continuing to be allowed to extract significant money out of people. Are they going to vote for candidates pushing actually effective measures to reduce how much people pay for medical care, if that means the stock will go down? Probably not.
I highly doubt OP actually did what they said they did, this was a SM post for publicity. Even if they did, they are absolutely in the minority, so there’s no reason to worry about public policy being impacted.
Because demand and supply don’t self-regulate healthcare. How much do you value your health? How about your own life? Oh, you’re willing to pay ANYTHING to live? Even if it’s not life threatening as long as it leaves you crippled, unable to work, you may as well be dead.
As a customer the only way to be an informed buyer is to be a physician yourself. Even if a treatment doesn’t work you still get charged, no refunds!
For-profit healthcare is fundamentally inhumane and is incompatible with capitalism. The forces that would usually regulate the market are non-existant. Demand is infinite, undercutting is pointless, customers have no way to be informed.
There’s a huge difference between emergency, life threatening care and relatively routine care. For example, if I need to get a tooth extracted, I can certainly wait to shop around a bit, and living with some pain for a few days could be worth finding a cheaper solution. I can also choose between hospitalization and self-care in many circumstances as well (e.g. normal baby delivery can happen at home or in the hospital).
For those cases where informed decisions are possible, supply and demand can work efficiently. It doesn’t work as well when there’s a monopoly on care, like in an ER, ambulances, etc.
And no, you don’t need to be a physician to be informed, you just need to consult one. I may not know the practical difference between operations, but I do understand chances of success and costs, and I know how to get multiple opinions and decide from there. That works for any field, I can convert a problem from needing an expertise to evaluating experts. Tell me what expected outcomes, the chances of various outcomes, and the costs, and I’ll get a second or third opinion if I’m not satisfied.
This gets even better the more transparent things are, because other experts can do independent reviews. A newspaper, for example, can hire a physician to review posted prices for routine operations and give an idea of how realistic those costs are. Insurance companies so exactly that, so I don’t see why a private organization couldn’t. News organizations routinely consult experts on stories.
But there are areas where there’s a monopoly, and those mess up the market’s ability to regulate prices. That’s why I’m in favor of universal coverage for emergency care, but against universal coverage for other forms of care.


{kind=link}
Why not? Companies that make pharmaceuticals, prosthetics, imaging devices, etc are all on the stock market too, so if hospitals weren’t on there, you could build a portfolio to approximate it by buying producers of medical equipment.
The real issue isn’t whether something is publicly traded, but collusion between groups to keep prices high. For example, it’s mutually beneficial for insurance, hospitals, and medical equipment providers to increase costs. Higher equipment costs means care providers can charge more (what’s another few hundred when the bill is in the thousands?), and higher total bills means insurance companies can charge higher premiums (they’re usually limited to a certain percent of cost as profit). Hospitals generally don’t have direct competitors since it’s prohibitively expensive to build one and there’s lots of bureaucracy based on “need,” so you can’t just go next door to an org that’s not involved in the collusion.
Here’s some YouTube videos about it:
There are lots of viable solutions here, but banning them from the stock market isn’t going to solve anything. The first order of business imo is making everything more transparent.
The real issue is the belief that essential services should make profit. Socialized, regulated Healthcare FTW.
I disagree.
I know it’s an anecdote, but I have a coworker that shared an experience moving from Canada to the US, and they said they much prefer the American healthcare system to the Canadian system. This is from the perspective of a relatively well off individual (not rich, just middle to upper middle class), so obviously someone at the bottom end of the income spectrum would have a different opinion.
So my question for people who promote socialized medicine is this: if you could easily afford both, would you prefer socialized or privatized medicine? And why?
I think we have a cost problem, not a structural problem, so we should look at ways of reducing cost before completely changing the structure of our healthcare system. My primary concern is getting insurance away from employers, publicly funding emergency services, and making hospital costs more transparent (e.g. publicly posted price ranges for common procedures). As in, reform the current system, not replace it.
The problem is that healthcare systems are meant to take care of the entire population, not just the middle class or higher. If you are a moderately healthy and wealthy person, yes the American healthcare system is fine, but that’s not exactly the what your entire system should be geared for.
The only reason they like the system is because they are the bread and butter of private insurance. Healthy working adults whom don’t require lots of expensive care. However, if they were to developed a chronic illness, or get injured or I’ll to the point where they can’t maintain their employment… That’s when you get to experience the worst healthcare experience America has to offer.
As someone who’s had socialized medicine (Tricare) and now currently has “good” private insurance (BCBS ppo), I definitely prefer socialized.
There’s no worry that your going to catch an unexpected co-pays, you aren’t nickle and dimed for every script or visit. No worrying about out of pocket maximums, yearly deductibles, or lack of specific coverage. You don’t have to get specialized insurance for just your eyes and teeth, the benefits go on and on.
The cost problem stems from the structural problem. Private insurance steals the ability to effectively collectively bargain for lower prices. It also diverts funding away from the socialized insurance pool of Medicare, which lacks the young healthy subscribers that help stabilize and fund the care for elderly and sick.
Imagine if all the money that private insurance pockets went towards actually caring for people. Imagine if hospitals didn’t have to employ a small army of managers and billing agents, just to get paid for services already rendered. Imagine the collective bargaining power that we’d all have if pharmaceutical companies knew there was only one customer in the entire nation.
You give that all away for what? A policy that goes away the moment your employer decides they don’t want to pay that much this year? A policy that ties your physical well being to your employment? A policy that terminates your coverage the very moment you need it the most?
Again, you’re talking about cost, not which you’d prefer from a service perspective.
I think there are lots of opportunities to make costs lower, such as reducing patent lengths (reduces medication costs) and simplify insurance (reduces admin costs). We should also make changes to liability law so doctors can focus on providing care. Some specific proposals:
And so on. And on top of that, expand Medicare/Medicaid a bit with costs phasing in the higher your income goes. I think we should also cap access to Medicare for retirees at a certain income level as well, and remove FICA tax caps.
We should absolutely be discouraging employer sponsored insurance and encouraging longer term insurance plans (e.g. like life insurance, you lock in at a lower rate if you sign up while healthy). Dropping someone from insurance shouldn’t be a thing at all, and the payout for doing so should be much higher than any costs the insurance company would incur by keeping them.
If you went to a restaurant and they ran separate charges every time you ordered something… You wouldn’t consider that bad service?
Also, I went to the same physician when on Tricare, so it’s the same exact service, minus all the billing hassle.
And I think you could do the same things and still lower the cost even more by banning privatized insurance?
Also, what is the profit motive for insurance companies to simplify their process? Their systems were purpose built to be as complicated and time consuming as possible, if they make the process easier, their subscribers would utilize it more, making insurance pay more often.
And again, why would corporations do this? And how would we enforce this?
The Medicare billing is automated, and pretty simple. It’s what every insurance company has the option of doing, but only Medicare and Medicaid have automated the process. This is because private insurance companies have no profit motive to pay for their prescribers healthcare.
Most hospitals have this information available, especially if you call their financial services office. In fact if you are a Medicare patient this information is publicly available on the CMS website, and they list exactly how they came to that figure.
The whole hidden ledger thing is primarily only a problem at privatized hospitals that were bought or built by private hospital networks operating for profit.
The inherent problem with this is that the elderly are fundamentally uninsurable. You can’t make a profit from an elderly subscriber, the cost of their end of life care will always cost more than any subscription fee they may pay in.
This is why the vast majority of private insurance do not offer primary insurance to people older than 65. The whole point of private insurance is to extract money from healthy patients and then dump them onto Medicaid if they become disabled, or onto Medicare when they begin to age and decline in health.
Who would offer those plans, and why? The only reason most people can afford private insurance is because their employer collectively bartered for the price. A lot of people have no idea how much of their employee compensation package is taken up by their insurance, but the burden of cost is redistributed by the entire employer pool.
This would bankrupt private insurance companies… I don’t think you fully understand how hard it is to make money on health insurance. The only way to do so is by withholding healthcare to your subscribers, or to offer plans with obscene co-pays or deductible.
The cost on average for full coverage is around 8.5k dollars a year for an individual, or 24k for a family. Meaning that the cost of a single operation, illness, or inpatient procedure will wipe away the potential profits from an individual subscriber for years. The only way to recover from having one I’ll subscriber is to balance them with a dozen healthy subscribers.
Without managing this equation of large healthy profitable pool vs small costly pool, the entire charade of private insurance would collapse upon itself.
One of the largest drivers in the increase in healthcare cost is these types of people. People whom don’t have any insurance, but still have healthcare needs. For these people the emergency room is typically their only option. This is one of the reasons emergency medicine is such a drain on hospital resources. For every person they treat without insurance, they have to raise the cost on people with insurance, simply so they don’t go out of business.
It’s funny you mention restaurants, in that case I don’t particularly care when they bill me because the menu says precisely what I’ll pay (counter order vs table service doesn’t matter as much as cost and quality). If it’s market rate (steak or seafood), they’ll tell me what the day’s rate is and what cuts they have.
I don’t get that with health care, even getting a range in a quote is like pulling teeth. I pushed back a ton when my daughter needed a surgery, and after several calls I still didn’t get a clear answer, and this was for a routine surgery. The quality and speed of service was great, billing was not.
One of the benefits of socialized medicine is not having to worry about billing, but you also often get delays in care. I don’t think we need to go to socialized medicine to solve the unexpected costs issue, we can expect care providers to absorb some of the variability.
I agree, the current profit motives are misaligned, and pushes like the ACA to further expand the number of people with insurance further entrench these practices.
The profit motive should be attracting customers who otherwise would go without. But since pricing isn’t transparent, cash payers don’t have the same leverage to get a fair price. Many care providers have an informal “cash discount,” but that’s just not the same.
If the system works well for cash customers, insurance would need to earn customers’ business, but when most people have insurance, the patient is no longer the customer, the employer is, so they’ll charge individual customers more than employers with group plans. If we separate the insurance from the employer, they would need to cater to patients.
Removing private insurance is one option, but that’s also quite disruptive and has potential for other issues (e.g. why would Medicare bother with good customer service if it’s the only option?).
That wasn’t my experience. We had two options for a surgery with different risks and costs, and after several calls, we couldn’t get any numbers, just A costs more than B. That’s why I’m so interested and “it depends on your insurance” blah blah blah. That’s why I’m so interested in this. And this wasn’t some podunk hospital, it was the premier children’s hospital in the state, run by the premier public university in the state, and services kids outside the state.
I should be able to get quotes on a procedure from multiple care givers for a non-urgent procedure (like the one we had).
Patients should be able to switch insurance if they don’t like the one they have. Right now, you either use the insurance you have or pay out the nose by giving up company cost share and ACA subsidies.
If my company offers a crappy plan, I should be able to take what they would’ve contributed and pick my own plan. If that was the case, insurance companies would try harder to make their service more convenient, just like auto insurance does (not a gold standard, but much better), and HR orgs would probably try harder to pick better plans.
If you’re wealthy, you don’t need much from your insurance. End of life care could be self funded, and insurance is there for the other surprises that could ruin your retirement. It would be totally acceptable for an insurance company to require some kind of down payment to cover EOL care, or a minimum number of years for coverage (if you die before the end of the contract, it counts as debt the estate needs to pay back).
I’ve run the numbers and can get a similar price (within 10% or so) for similar coverage without ACA subsidies, but I need to factor in how much they’d contribute to their own plan. Add to that couples who both work, your options are: have separate plans (less efficient) or give up the employer subsidy.
No, they’d just adjust rates to compensate. If there’s something insurance companies are good at, it’s averaging costs and holding a surplus. So a company that’s better able to estimate this should get more customers and stay in business longer.
If they offer a 10-year or longer plan, they just need to average costs across their target demographic over those years to come up with a premium. Term life insurance companies do this, so why not health insurance?
Especially for homeless people. Which is a huge part of why I’m a fan of government funded ER. That’s a huge risk factor for insurance companies and hospitals, and it’s also a huge complexity for visitors and whatnot, so it should just be provided. If the paramedic thinks you need emergency care, it should be 100% free. However, hospitals should be empowered to deny care (and charge for wasting ER capacity) for non-emergencies.
But any extended care once you’re stabilized should be covered by insurance instead, because you have actual choices in your care (and could theoretically walk out if you choose not to accept further care).
We were talking about service, not cost… Like if they ran your card for every individual item, as soon as you ordered it. “I’d like to start with a coke to drink” takes out card to charge. “Then I’d like a starter” takes out card.
This is what i mean by bad service.
This is likely because you called before a prior authorization was completed, meaning that you most likely were utilizing private insurance. If you were utilizing Medicaid, which doesn’t require pre authorization, then it would be really simple to tell you.
You can’t give an accurate quote for private insurance because the individual plans are so personalized by their workplace or insurance brokers to lower cost and coverage that we literally don’t know what your coverage until we submit if for authorization and equate for things like deductables and copay.
This authorization process requires not only a referral, but an itemized script, supporting notes, and a face to face with the provider. So unless they had the opportunity to complete these task, private insurance doesn’t allow us to give you a quote.
Lol, you were just talking about a delay in care due to billing issues with private insurance. American private insurance also has the same exact delays in care, waiting weeks for prior auth, waiting months for people to meet their deductible, avoiding needed care because of cost, and just plain waiting for specialized care because we don’t have enough specialty providers. Many specialty providers like neurologist or or rheumatologist have left the field specifically because of paperwork burnout. The authorization process for these expensive specialty practices is so scrutinized by insurance companies that it can take months of daily negotiation to even see a patient.
Lol, wrong again. The plans allowed on the aca marketplace had to follow aca guidelines, which included automating the billing process. These platinum, silver, and bronze plans are actually pretty easy to work with compared to those offered by people’s workplaces. In the beginning we were actually pretty excited to see actual changes to the system, however since the removed mandate, and the subsequent deterioration of coverage in these plans, it’s rare to see patient actually utilize there benefits.
What are you talking about about? Why would an insurance company want to attract uninsured people? The uninsured people of America are some of the most at risk communities in America. They are impoverished, underemployed, and are disproportionately likely to have long term health conditions. There is no wealth to extract from these people, and the longer they have been uninsured, the more likely they are to require excessive care once they are insured.
Lol, you have no idea the average cost of healthcare people accumulate during their lifetimes. One serious stint at an inpatient facility would bankrupt a wealthy person. As I said, there is no profit in healthcare that isn’t created by denying healthcare.
Why exactly would it be quite disruptive? Also, Medicare is the only option for the people who have it… If you qualify for Medicare for your primary insurance, private insurance automatically becomes your secondary. Medicare still offers more coverage than any other private plan. I don’t think you quite understand that the people whom work in healthcare do so because they want to help people. Being a physician doesn’t exactly mean you’re making the big bucks anymore. There are plenty of fields that require a lot less schooling and pay way more.
As I said previously, this is an inherent problem created by private insurance. You can’t just call and shop around on private insurance, the way they set up the prior authorization process is expressly made to prohibit this. The only way to do this is to call your insurance as a subscriber, and talk to your plans agent. They will direct you to their preferred network, where they have negotiated cost previously.
Again, insurance companies purposely create inefficient and archaic systems so their customers won’t utilize their services as often. They make us do all the explaining and processing, so we get the blame.
I agree, and if your child was on Medicaid it would have been super easy… You would have been told $0.00. Medicaid is an actual healthcare system, and because their goal is to actually improve their patients health it functions as intended.
Right, but who is preventing people from switching plans… Oh yeah, private insurance. Because private insurance cannot afford to have patients switching insurance every time a patient has an operation. How are you going to remain solvent if a subscriber can just run up cost and then switch to a different insurance pool without contributing?
You are ignoring the fact that private insurance is a gamble. It’s a company gambling that you as an individual will contribute more to the insurance pool than you take out before you turn 65. If a person can just switch insurance companies they could just change plans every year they needed an expensive operation. The same can be done with home/car insurance, but car/home insurance is allowed to charge people with prior history of heavy utilization with higher fees and deductible. This is not legal in healthcare, as it would automatically price out people with chronic illnesses.
And how many people are wealthy compared to the amount of people who are poor? Is your solution to build the entire country’s healthcare system for 5% of the population? Also, why should your life savings be eaten up by healthcare cost if you already paid for life insurance your whole life? I just don’t see why you are so ardent about paying more money for less coverage?
You are comparing individual self funded plans to those offered by your work? As someone who owns a company and works for a hospital… I highly doubt that. I’m still utilizing my hospital insurance because the self funded ones offered to small companies were quite a bit higher when factoring in deductible and copays. If you were talking about individually funded plans, I would urge you too re examine the coverage.
The amount they would have to raise rates exceeds their clients ability to pay… You can’t squeeze blood from a stone, and people are already struggling with their current cost. Raising the rate high enough to account for chronic disabilities isn’t an option. This is why they fought so hard against the law that prevented them from rejecting coverage for people with conditions like type 1 diabetes, which isn’t a disability that qualifies for Medicaid, but has a high cost.
That’s just a bandaid who’s only function is to protect insurance companies. If insurance companies are not good enough to cover emergent healthcare what’s their point? If you can get free healthcare at emergency rooms instead of being insured, why not just go to the ER? This would just make the emergency room problem worse.
Why spend so much time coming up with worse work arounds when you haven’t been able to tell me a single advantage private insurance brings to the table?
I’m not really following the point of the analogy.
If cost doesn’t matter, I’d just give them my card and they can run it as often as they like. That’s basically how it works on cruise lines, you set up a payment system and they scan your cruise card with each transaction. It’s not an issue at all.
Right, and that’s because the policy holder usually isn’t the customer, the employer is.
Health insurance would likely be a lot simpler if the average policy holder could switch insurance, especially if there’s no open enrollment period (like car insurance, I can shop rates anytime and understand what I’m buying pretty easily).
No, there was no delay in care. Once I picked the option, I got the procedure done in the next week or two.
The only delay was because I wanted the quote before picking the solution, and that’s a totally artificial limitation that can be fixed by changing how insurance works (i.e. give me the cash price, and I’ll figure in the deductible and whatnot).
You’re right, the problem is paperwork, which is why we should give the insurance companies fewer options to reject claims. Eliminate or automate the authorization step. Care providers should never need to talk to anyone at the insurance company.
Higher risk just means higher costs. They can still collect some percentage of premiums, so why would they turn it down?
You’re right, and those numbers are hard to come by since most studies/articles assume Medicare in retirement and focus on out of pocket costs. If I was proposing actual policy, I’d do my due diligence, but for this kind of discussion, I use what’s readily available.
65+ insurance is indeed unique, hence why I mentioned an escrow system. Basically, you prepurchase insurance including end of life care. That amount of money buys you a certain guaranteed tier of end of life care, even if your individual costs exceed that. I’m guessing that escrow is something like $300-500k for basic EOL care, plus some extra for routine medical care. But I only have mediocre data to work from. If you have a good source, I’m interested.
I don’t know how practical it is, it’s just an idea for an alternative to Medicare for the wealthy. But honestly, just uncapping income for paying in and expanding Medicare a bit for poorer people is probably more reasonable.
Sure, and the same is true for education. And the problems with both are pretty similar:
In many areas, the government has a near monopoly on education, yet the problems persist. Why should we expect medicine to be much different? Once government has a near monopoly on something, it becomes very political.
Maybe something like the public option doesn’t have as many tradeoffs, IDK, but socialized medicine certainly would. I’d only be in favor of a public option if care providers received the same amount from cash customers vs Medicare customers, and that amount is transparent and publicly auditable (i.e. if Medicare wants to fight high prices, that should benefit cash customers). That doesn’t happen today with the privatized system, so that’s where my focus is.
Privatized insurance isn’t the goal here, privatized medicine is. If we want to subsidize that for the poorer end of the income range, I’m fine with that, but the majority should be expected to pay for a large portion of medical care, otherwise market forces don’t work properly.
They do it because it doesn’t cost them customers. I can’t vote with my wallet and switch my insurance, I can only beg my HR department to offer something different. I am not the customer here.
Many customers are willing to pay a bit more in other industries to avoid BS, I don’t see why that should be any different for health insurance.
The reason we have the system we do is because government incentivizes company-provided health insurance. We should instead encourage people to select their own plans. The ACA increases barriers to rejecting company insurance and doubles down on involving employers in health insurance decisions.
Either we need to completely put patients in control of their insurance or provide it as a public good. The current middle ground is worse than either extreme imo.
Auto insurance seems to work just fine with this. If I make lots of claims with one insurer, that slate won’t just be wiped clean with the next one.
If customers can easily switch, that should encourage insurance companies to lock in customers with longer term policies to spread out the risk.
And insurance isn’t really a gamble, it’s actually quite the opposite, a way to reduce risk. The insurance company doesn’t expect any particular individual customer to be profitable, they just expect that their customers will be profitable on average. Individuals buy insurance knowing that they statistically don’t get value from the insurance, they’re merely getting it to reduce their own financial risk. For an insurance company, it’s like buying an index fund instead of individual stocks, and for individuals it’s like buying an annuity instead of stocks.
Yes. I’m comparing individual, non-subsidized ACA plans with those offered by my work. My work only offers high deductible plans with a premium and HSA contribution, and I’m comparing against ACA HSA plans with a similar deductible and max out of pocket. I’ve never had a copay, everything has been a relatively simple deductible.
Specific details certainly differ, but I think it gets me in the ballpark.
And this is for a reasonably large company. We have something like 3000 employees, so it should be big enough to benefit from collective bargaining. I haven’t run the numbers for a couple years (I compared ACA when self-employed vs new company), so things could have changed. I like this method because costs are both transparent, and I actually estimate my costs (and subsidy) if i decide to stop working in a spreadsheet. I’m certainly no expert, but I do try to be reasonably thorough.
And yeah, I’ll probably redo the numbers soon. I generally do this around tax season because I like to estimate my taxes to see how close I am (was really close last year), and I have a section to compare expected total costs of care for the two plans my company offers (only difference is deductible, premium, and max out of pocket) and a comparable ACA plan (those numbers are publicly available). Specific plan details vary, and it’s not something I can get super accurate with (how do you put a price on a procedure I’m unlikely to need?), but hopefully it’s close.
If you’re interested, maybe I’ll run the numbers this weekend and reply with the details. I’m not a medical or insurance expert, but I am very interested in personal finance and actually enjoy spending a few hours crunching numbers.
Maybe. But that’s also assuming healthcare costs stay stagnant. If we drastically reduce the complexity of dealing with insurance, we also reduce the costs to insurance, which may be enough to offset an increase in claims.
All the paperwork is waste, and it’s getting to be a massive problem, but it suffers from a prisoner’s dilemma-type issue (an individual company is better off complicating the process in the short term, but if everyone does that, net costs go up) so the current setup won’t resolve itself.
Insurance companies exist to cover extreme financial burdens, like developing cancer or other chronic conditions. Basically, things that could bankrupt you.
The issue with ER is that it often goes against your will, and getting financial consent could be the difference between life and death. What are you going to do if insurance rejects your claim? What if someone else calls an ambulance for you and you can’t pay? What if you’re a tourist and you don’t understand the US medical system? There’s just way too many weird cases to the point where we can’t just expect insurance companies to take the hit here.
Publicly funded ER solves those problems and can protect emergency care providers from lawsuits and whatnot so they can focus on providing care. Once the patient is stabilized, they can make decisions for ongoing care, and that’s where insurance should get involved.
In general, if something is involuntary or a natural monopoly, it should be publicly provided. That’s absolutely the case for emergency care (I can’t pick the ambulance company someone else calls for me). But routine and chronic care absolutely is voluntary and isn’t a natural monopoly.
The ER would reject you and potentially fine you for nonemergency care. Just like calling 911 for non-emergencies.
This isn’t how pricing is set for medical equipment… Nor is high equipment cost the reason behind the pricing increase.
Every hospital that accepts Medicare utilizes CMS guidelines when it comes to billing. Medicare sets the general price for items, factoring in things like historic pricing, cost of purchase from vendor, and the price of labour required to fit or make the device function.
The complex and expensive aspect of hospital billing stems from the introduction of private insurance companies. The ones that require more paperwork and processing time than Medicare, and will attempt to make the process as hard as possible.
Because hospitals are a natural monopoly, not only are they prohibitedly expensive, but it’s also extremely hard to profit from them in the long term. Which is why there’s a large amount of bureaucracy to get them built.
Pretty much every ER room in America is a huge money sink that the rest of the hospital has to economically support. You add too many hospitals, and the services that are profitable get too spread across the area to support their individual ER operations.
Which is why about 10-15 years ago there was a large push from venture capital to build “hospitals” without trauma rooms. These hospitals began to eat up all the funding in the area and began shutting down hospitals with trauma wards. This is when a lot of states adopted legislation that would help curb this behavior.
Banning private insurance is the only thing that would lower prices for Americans. None of the issues you covered are even close to the reason why things are getting expensive.
Not when there’s any kind of population density.
But what are those insurance companies processing? If you look at it, it’s “special deals” so the agents can get a bonus, it has nothing to do with actually saving their customers money. Hospitals inflate prices so they have room to make cuts so the insurance sales people feel like they’re winning.
The problem here isn’t with the nature of insurance, but the collusion between insurance companies and care providers. It’s a dance they play so everyone feels like they’re winning, and at the end of the day the customer is the one that loses. It’s not a competitive market, it’s a bureaucratic one where you have HR departments, insurance salespeople, and hospitals all propagating the current system because it’s lucrative for all of the middlemen.
Medical suppliers want a piece of the action too. That’s why we get things like insulin prices going up:
They prevent competition through the patent and regulatory systems, and hospitals and insurance companies are fine with it because they just pass the costs on to the consumer. Consumers don’t really have a choice because most insurance comes from employers (who just pay employees less to compensate) or taxes (ACA subsidies). Nobody actually pays the full price, so the system continues.
The same goes on with medical devices, but volume is much lower so it’s easier to prevent real competition. Add to that the legal risk for choosing a cheaper product if anything goes wrong and you’ll find no incentive to cut costs.
Let’s assume we eliminate private insurance, you just change the private collusion to public collusion, and instead of middle managers getting paid in the public sector, you get political favors to keep prices high (e.g. campaign donations). Moving insurance from private to public just moves money from one pocket to another. The true solution here is to expose the collusion, not politicize it. If you want proof of this in action, look no further than the defense department in the US.
Which is because of free riders. The solution to that problem is different: emergency care should be completely publicly funded. It’s so expensive because the hospital has to deal with people skipping on their bills and just move the costs to paying customers.
I think we should make ambulances and all non-elective care completely free, provided a paramedic recommends emergency care.
Natural monopolies aren’t intrinsically changed by demand…
It’s not the insurance company that is doing the processing. It’s the hospitals, they have to hire more and more billing agents just to extract the money that the insurance has already agreed to pay.
Lol, no. By “special deals” you mean 20% less than the Medicare allowable, and if you don’t agree then you are no longer in network.
No, they inflate the prices so that when insurance companies ask for less money it doesn’t bankrupt the hospital.
You have no idea what you are talking about about… I’m a provider at a hospital, specializing in orthopedics and rehabilitation. I’ve never spoken to an insurance agent about pricing. That’s not how it works.
Those are pharmaceutical companies, not medical suppliers, they are billed under completely different systems…
Also, the reason insulin pricing is so high is because Medicare isn’t allowed to barter for pricing, largely in part because it would be unfair to private insurance companies who have smaller subscriber groups.
Oh yeah, I forgot how every medical system on the planet was completely fraudulent… Oh wait, nope, mainly just America.
The biggest way to improve pricing is by group bartering, which is how every other 1rst world nation pays less for medical equipment, treatment and prescription cost than the US.
Again, nothing you said was accurate, and anyone who takes it as so is now dumber than when they began reading. Please stop spreading misinformation about fields of study you do not specialize in.
Market competition is fine, but corporations are specifically obligated to focus on profits over other considerations, and in this case that is inappropriate and creates perverse incentives. Consider people like in the OP who have cynically bought in (or are in some retirement fund that bought in on their behalf) and now their financial wellbeing depends on hospitals continuing to be allowed to extract significant money out of people. Are they going to vote for candidates pushing actually effective measures to reduce how much people pay for medical care, if that means the stock will go down? Probably not.
I highly doubt OP actually did what they said they did, this was a SM post for publicity. Even if they did, they are absolutely in the minority, so there’s no reason to worry about public policy being impacted.
Because demand and supply don’t self-regulate healthcare. How much do you value your health? How about your own life? Oh, you’re willing to pay ANYTHING to live? Even if it’s not life threatening as long as it leaves you crippled, unable to work, you may as well be dead.
As a customer the only way to be an informed buyer is to be a physician yourself. Even if a treatment doesn’t work you still get charged, no refunds!
For-profit healthcare is fundamentally inhumane and is incompatible with capitalism. The forces that would usually regulate the market are non-existant. Demand is infinite, undercutting is pointless, customers have no way to be informed.
There’s a huge difference between emergency, life threatening care and relatively routine care. For example, if I need to get a tooth extracted, I can certainly wait to shop around a bit, and living with some pain for a few days could be worth finding a cheaper solution. I can also choose between hospitalization and self-care in many circumstances as well (e.g. normal baby delivery can happen at home or in the hospital).
For those cases where informed decisions are possible, supply and demand can work efficiently. It doesn’t work as well when there’s a monopoly on care, like in an ER, ambulances, etc.
And no, you don’t need to be a physician to be informed, you just need to consult one. I may not know the practical difference between operations, but I do understand chances of success and costs, and I know how to get multiple opinions and decide from there. That works for any field, I can convert a problem from needing an expertise to evaluating experts. Tell me what expected outcomes, the chances of various outcomes, and the costs, and I’ll get a second or third opinion if I’m not satisfied.
This gets even better the more transparent things are, because other experts can do independent reviews. A newspaper, for example, can hire a physician to review posted prices for routine operations and give an idea of how realistic those costs are. Insurance companies so exactly that, so I don’t see why a private organization couldn’t. News organizations routinely consult experts on stories.
But there are areas where there’s a monopoly, and those mess up the market’s ability to regulate prices. That’s why I’m in favor of universal coverage for emergency care, but against universal coverage for other forms of care.